| |
Chiropractic manipulative therapy with helmet therapy, association with treatment duration and cranial asymmetry outcomes for moderate to severe positional plagiocephaly: a retrospective cohort study
Adam Sayers, MTech Chiropractic, MScMPH
Chiropractor in private practice
Health Sciences University
Johannesburg, South Africa
Aurélie M Marchand, MChiro, MScACPP, MMEd
Course Leader, MSc Musculoskeletal Paediatric Health
Health Sciences University, AECC School of Chiropractic
Bournemouth, United Kingdom
Alister DuRose, MChiro, PhD
Senior Lecturer in Clinical Sciences
Health Sciences University, AECC School of Chiropractic
Bournemouth, United Kingdom
Adam Sayers, Corresponding Author
218 Voortrekker Road, Monument, Krugersdorp
Phone: +27798947401
Email: drchiroadam@gmail.com
ABSTRACT
Objectives: This study aimed to determine whether the inclusion of chiropractic manipulative therapy (CMT) during helmet therapy reduced the treatment duration and improved measurement outcomes for infants with moderate to severe positional plagiocephaly. Methods: This was a retrospective cohort study using clinical records from a South African orthotist. Infants aged 4–12 months with moderate to severe nonsynostotic plagiocephaly were divided into two groups: those who received helmet therapy alone (control) and those who received helmet therapy combined with CMT (intervention). The primary outcome was treatment duration (weeks); secondary outcomes included changes in cranial vault asymmetry (CVA) and cranial vault asymmetry index (CVAI), measured using SmartSoc® 3D scanning technology. Results: Of the 128 eligible infants, 61 families responded and gave consent, 24 infants met the inclusion criteria (12 control, 12 intervention). The mean treatment duration showed no significant difference between groups. However, the intervention group achieved significantly better cranial symmetry outcomes, with final CVA (p = .010) and CVAI (p = 0.010) values lower than the control group and more change for both CVA (p = .755) and CVAI (p = .693) than the control group. Conclusions: While the addition of CMT did not shorten the duration of helmet therapy, it was associated with superior cranial symmetry outcomes at discharge, potentially indicating more efficient symmetry correction. These findings suggest potential added value in combining CMT with helmet therapy in improving cranial symmetry. Further prospective studies with larger samples and standardized chiropractic protocols are warranted to confirm these preliminary observations.
Keywords: Chiropractic, manual therapy, plagiocephaly, helmet therapy, orthotic devices.
Introduction
Positional plagiocephaly (PP) is an asymmetrical deformation of the infant skull resulting from prolonged external pressure on the pliable neonatal cranium, in the absence of craniosynostosis.1,2 The condition is most commonly associated with prolonged supine positioning, often combined with positional head preference.2,3 Additional risk factors include first-born status, multiple gestation, assisted or traumatic delivery, congenital muscular torticollis, intrauterine growth restriction, and insufficient prone (“tummy time”) positioning.3-5 Since the introduction of the “Back to Sleep” campaign in the early 1990s, the incidence of positional plagiocephaly has increased by an estimated 400–600%.4,6,7,8 Current prevalence estimates range from 20% to 40%, making it the most common positional cranial deformity in infancy.9,10 This substantial rise has led some authors to describe PP as a growing public health concern or “pediatric epidemic”.11
Clinically, positional plagiocephaly typically presents as a parallelogram-shaped head, characterized by unilateral occipital flattening, ipsilateral anterior ear displacement, frontal bossing on the same side, and contralateral parietal prominence.2,9 More severe cranial asymmetries have been associated with longer-term consequences, including orthodontic abnormalities, mandibular asymmetry, and temporomandibular joint dysfunction.3,12,13 Associations with delays in motor development, language, cognition, visual field restriction, malocclusion, and muscular dysfunction have also been reported.3,12,13 Infants with cranial vault asymmetry (CVA) greater than 10 mm, classified as moderate to severe, demonstrate a significantly increased association with developmental delays.14 These concerns highlight the importance of early and effective conservative management strategies.15
Conservative treatment options for PP include repositioning strategies, physiotherapy, massage therapy, manual therapy, and helmet therapy.4 A recent systematic review by Blanco-Díaz et al.15 concluded that pediatric physical therapy programs should be considered the primary initial intervention, and that the inclusion of manual therapy leads to superior improvements in cranial measurements compared to caregiver education alone.9,16,17 Helmet therapy is considered a low-risk and effective intervention for moderate to severe plagiocephaly, particularly when conservative measures have failed.2,6,10 Its effectiveness is strongly age-dependent, with optimal outcomes achieved when initiated before six months of age, although sufficient head and neck control is typically required.2,6,11 Helmet therapy is generally recommended before twelve months of age due to diminishing cranial growth thereafter.4,8
While the concurrent use of physiotherapy or manual therapy alongside helmet therapy has been suggested in moderate to severe cases,7,12 the literature remains unclear regarding the effectiveness of simultaneous treatment. To date, only one study has explicitly investigated concurrent manual therapy and helmet therapy, demonstrating a reduction in helmet treatment duration in severe plagiocephaly.18 There is currently a lack of research examining the role of chiropractic manipulative therapy (CMT), adapted to the infant, as part of a combined treatment approach.
Manual therapy within the plagiocephaly literature primarily refers to physiotherapy or osteopathic interventions, with limited chiropractic-specific investigation.3,4,6,9,15,16,18,19 Chiropractic care emphasizes manual therapy as part of a treatment protocol in pediatric populations.20 In South Africa, chiropractors demonstrate positive engagement with evidence-based practice,21 and parents commonly seek chiropractic care for infants, particularly for conditions such as torticollis and cranial asymmetry.22 Despite this, chiropractic-specific reports for the treatment of plagiocephaly and higher quality research remains limited.
The aim of this study was to assess whether the addition of chiropractic manipulative therapy is associated with reduced helmet therapy duration and improved cranial measurement outcomes in infants with moderate to severe positional plagiocephaly. It was hypothesized that the inclusion of CMT alongside helmet therapy would result in shorter treatment duration and improved cranial asymmetry measurements compared to helmet therapy alone.
Methods
Study design and setting
A retrospective cohort study design was used to compare outcomes between infants who received helmet therapy alone and those who received helmet therapy combined with chiropractic manipulative therapy (CMT). This design was chosen as participants were grouped according to exposure status rather than outcome status. The study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.23
The study was conducted using clinical records from a private orthotic practice in South Africa, where documentation routinely includes whether infants underwent chiropractic care during helmet therapy. This enabled comparison of helmet therapy duration between an exposed group (helmet therapy with CMT) and an unexposed control group (helmet therapy alone). Recruitment occurred over an eight-week period from March to May, 2025. Parents of eligible infants were contacted via telephonic messaging. Ethical approval was obtained from the Health Sciences University (United Kingdom; SOC-1024-009) and the Durban University of Technology (South Africa; IREC 006/25).
Participants and eligibility criteria
The orthotist screened records to identify infants who had received cranial orthoses specifically for nonsynostotic positional plagiocephaly, excluding other cranial deformities and craniosynostosis. Parents of 128 infants meeting these criteria were invited to participate. The invitation included study information, consent to access clinical records, and a request for infant demographic details.
Infants were eligible if helmet therapy was initiated between 4 and 12 months of age and if plagiocephaly severity was classified as moderate or severe based on cranial vault asymmetry (CVA) and cranial vault asymmetry index (CVAI) criteria (Table 1). Infants outside the age range or with mild or normal asymmetry were excluded.
Severity classification
Normal
Mild
Moderate
Severe |
Crainial vault asymmetry (CVA) classification
< 5mm
5 – 10mm
10 – 15mm
> 15mm |
Crainial vault asymmetry index (CVAI)
< 3.5%
3.5 – 6%
6 – 10%
> 10% |
Table 1: Severity classification of positional plagiocephaly adapted from Kim et al.2
Outcomes and variables
The primary outcome was duration of helmet therapy, measured in weeks from initiation to discharge as determined by the orthotist. Secondary outcomes included changes in CVA and CVAI from initial to final measurements. The exposure variable was receipt of CMT during the helmet therapy period. Participants were assigned to the control group if they received helmet therapy alone or to the intervention group if they received helmet therapy combined with CMT. Other variables considered as potential predictors included age at initiation of helmet therapy and initial severity of asymmetry. No formal interaction testing was conducted, and no data on adverse events were collected.
Data collection and measurements
Following informed consent, demographic data including date of birth and sex were collected from parent surveys. Measurement data and scan dates were obtained from the orthotist’s clinical records. Helmet therapy duration, age at initiation, and age at discharge were calculated using these dates. All data were recorded on a standardized data extraction sheet prior to analysis. Cranial measurements were obtained using a SmartSoc® 3D scanner with Ebrace software, which calculates CVA and CVAI for each scan (Figure 1). CVA represents the difference between the two diagonal cranial measurements, while CVAI is calculated as CVA divided by the shorter diagonal length and multiplied by 100 to yield a percentage. CVAI allows for standardized comparison across infants with differing head sizes and was included alongside CVA as an outcome measure.2,8,9,25
The SmartSoc® system permits infant movement during scanning and reports measurement accuracy to 0.01%, minimizing concerns regarding measurement error.26 All cranial orthoses used were STARband® helmets manufactured under U.S. Food and Drug Administration regulation by Orthomerica.
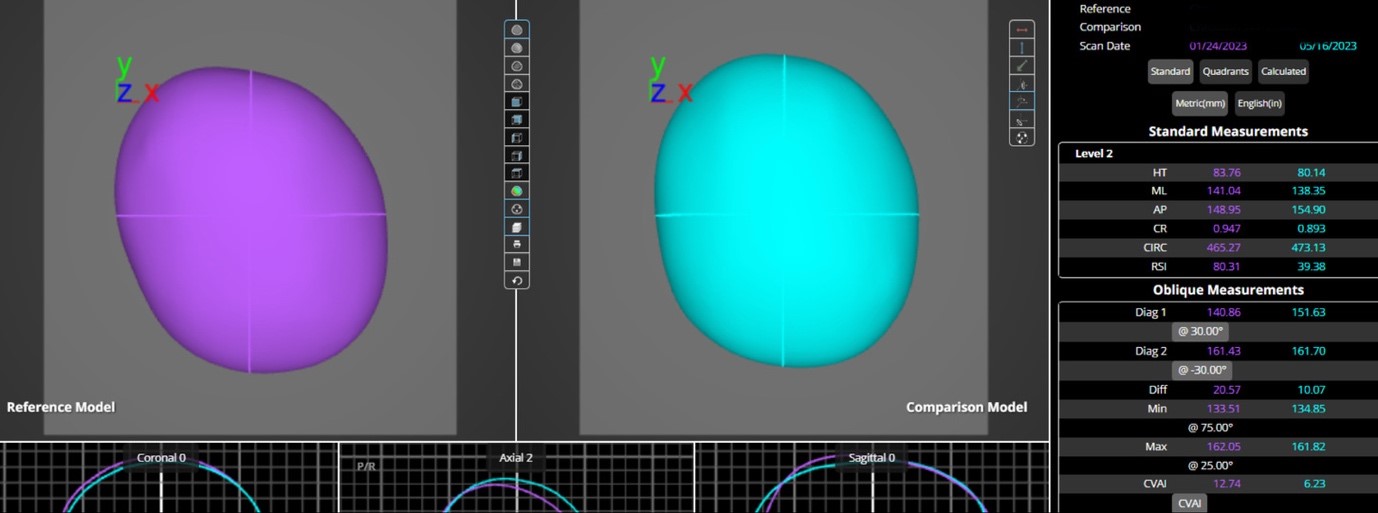
Figure 1: Comparison between initial (purple) and final (green) measurements collected from the orthotist, performed with SmartSoc® 3D scanner, and analysed on Ebrace software.
Helmet therapy protocol
Helmet therapy followed a standardized orthotic protocol, including gradual daily increases in wear time to a maximum of 23 hours per day, with follow-up assessments every three to four weeks. Treatment cessation was determined by the orthotist when CVA was reduced to less than 6mm, typically within the normal severity range. Helmet therapy concluded earlier if treatment goals were achieved before 12 weeks or continued beyond this period if necessary. For this study, helmet therapy duration and changes in CVA and CVAI were compared between the control and intervention groups.
Sample size
A convenience sample was used due to the retrospective nature of the study and reliance on available clinical records from a single orthotic practice. Of the 128 infants who received helmet therapy for positional plagiocephaly, all cases meeting inclusion criteria and with complete data were included in the analysis.
Statistical analysis
Statistical analysis was conducted using IBM® SPSS® Statistics (version 30.0). Quantitative variables included age at initiation of helmet therapy, duration of helmet therapy (weeks), and cranial vault asymmetry (CVA) and cranial vault asymmetry index (CVAI) at initiation and discharge. Data distributions were assessed using the Kolmogorov–Smirnov test and were normally distributed. Descriptive statistics are reported as means with standard deviations. Group comparisons between the control and intervention groups were performed using independent samples t-tests. For each comparison, t statistics with degrees of freedom, 95% confidence intervals, and p values are reported. Statistical significance was set at p < 0.05. No subgroup or interaction analyses were performed. No missing data or loss to follow-up occurred.
Results
Participation and participant characteristics
Figure 2 illustrates participant flow and baseline characteristics. Of the 128 eligible infants, 61 parents (47.6%) provided consent. Thirty-seven infants were excluded due to mild plagiocephaly, resulting in a final sample of 24 participants. The cohort included 13 males (54.2%) and 11 females (45.8%).
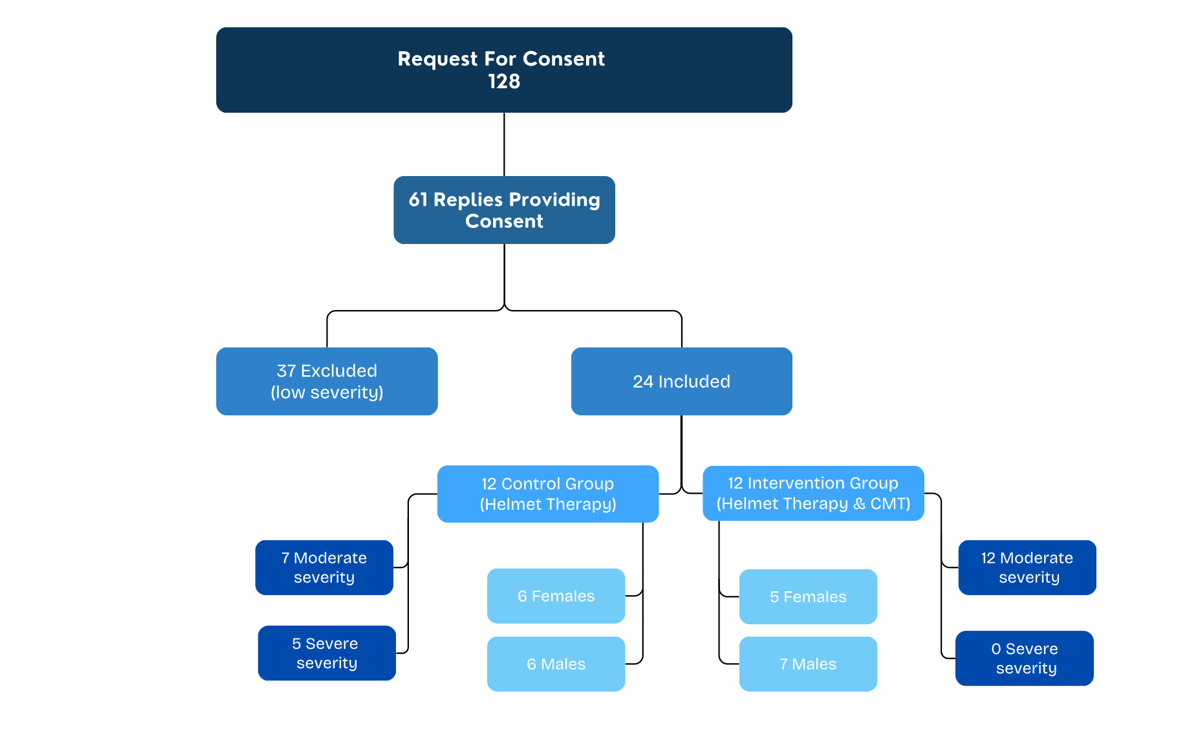
Figure 2: Flow diagram demonstrating recruitment, participation numbers, numbers of male and female participants per group and severity distribution between groups.
Twelve infants received helmet therapy alone (control group) and 12 received helmet therapy combined with chiropractic manipulative therapy (intervention group). The control group comprised 7 infants with moderate and 5 with severe plagiocephaly, while all infants in the intervention group presented with moderate severity at baseline. Sex distribution was balanced between groups, with 6 males and 6 females in the control group and 7 males and 5 females in the intervention group.
Baseline measures
The mean age at initiation of helmet therapy for the total sample was 6.00 months (SD = 1.60). Mean initiation age was 5.54 months (SD = 1.30) in the intervention group and 6.46 months (SD = 1.79) in the control group, with no statistically significant difference between groups (p = 0.166) (Table 2).
| Characteristics |
Control Group (Helmet Only)
Mean ± SDa |
Intervention Group (Helmet + CMT)b
Mean ± SD |
t and p Values |
Initiation age
Duration (weeks)
CVAc initial (mm)
CVA end (mm)
CVAId initial (%)
CVAI end (%)
CVA change (mm)
CVAI change (%) |
6.46 ± 1.79
13.92 ± 3.68
14.23 ± 3.08
6.04 ± 2.56
9.59 ± 1.92
3.98 ± 1.63
8.19 ± 3.29
5.61 ± 2.14 |
5.54 ± 1.30
14.17 ± 3.43
12.06 ± 1.73
3.52 ± 1.74
8.26 ± 0.91
2.37 ± 1.15
8.54 ± 2.14
5.90 ± 1.22 |
t(22) = 1.43, p = 0.166
t(22) = -0.17, p = 0.865
t(22) = 2.13, p = 0.045
t(22) = 2.83, p = 0.010
t(22) = 2.16, p = 0.047
t(22) = 2.80, p = 0.010
t(22) = -0.32, p = 0.755
t(22) = -0.40, p = 0.693 |
Table 2: Demographics and clinical characteristics of participants in the control and intervention groups.
At initiation of therapy, mean cranial vault asymmetry (CVA) was 14.23 mm (SD = 3.08) in the control group and 12.06 mm (SD = 1.73) in the intervention group, representing a statistically significant difference (t(22) = 2.13, p = 0.045; 95% CI [0.05, 4.28]). Mean cranial vault asymmetry index (CVAI) at initiation was 9.59% (SD = 1.92) for the control group and 8.26% (SD = 0.92) for the intervention group, also demonstrating a statistically significant difference (t(22) = 2.16, p = 0.047; 95% CI [0.05, 2.60]). According to these means, both groups were classified within the moderate severity category at baseline, with the control group at the higher end of the moderate category range.
Treatment duration
Mean duration of helmet therapy for the total sample was 14.04 weeks (SD = 3.48). Mean duration was 13.92 weeks (SD = 3.68) in the control group and 14.17 weeks (SD = 3.43) in the intervention group. The difference in treatment duration between groups was not statistically significant (t(22) = –0.17, p = 0.865; 95% CI [–3.26, 2.76]) (Table 2).
Secondary outcomes
Pre- and post-treatment CVA and CVAI values for both groups are presented in Table 2. At discharge, mean CVA and CVAI values were lower in the intervention group compared to the control group. The intervention group demonstrated statistically significantly lower CVA and CVAI values at discharge relative to the control group. Changes in CVA and CVAI from initiation to discharge were greater in the intervention group compared to the control group; however, these differences in magnitude of change were not statistically significant.
Discussion
The primary aim of this study was to determine whether the inclusion of chiropractic manipulative therapy (CMT) during helmet therapy for moderate to severe positional plagiocephaly was associated with a reduction in orthotic treatment duration. The findings demonstrated no statistically significant difference in helmet therapy duration between the control group and the intervention group, with mean treatment durations of 13.92 weeks and 14.17 weeks, respectively. This suggests that the addition of CMT did not influence the overall length of helmet therapy. Despite the absence of a duration effect, differences were observed in cranial asymmetry outcomes. The intervention group demonstrated significantly lower mean CVA and CVAI values at discharge compared to the control group and achieved values within the normal severity category, whereas the control group remained within the mild category. Although the magnitude of change in CVA and CVAI was slightly greater in the combined therapy group, these differences were not statistically significant. These findings suggest that while CMT did not shorten helmet therapy duration, it may have contributed to improved cranial symmetry outcomes in this cohort.
The lack of significant treatment duration effect contrasts with a prior study reporting reduced helmet therapy duration when manual therapy was used concurrently.18 However, that study employed a standardized manual therapy protocol and did not report objective cranial asymmetry measurements, limiting direct comparison. Helmet therapy duration is largely dependent on infant cranial growth rate and orthotist-defined treatment protocols,2,8,25 factors that are unlikely to be directly influenced by CMT or other manual therapies. Additionally, the orthotist involved in this study adheres to a standardized protocol of approximately 12 weeks or longer, consistent with existing literature recommending a minimum of three months for effective correction.2,10
While CVA is commonly used in clinical practice, CVAI allows standardized comparison across infants with differing cranial sizes.2,8,9,24 In this study, the intervention group demonstrated lower discharge CVA and CVAI values. Interpretation of these findings is limited by baseline differences, as the control group presented with significantly greater initial severity. Initial severity is a recognized predictor of helmet therapy outcomes, with less severe cases generally achieving lower residual asymmetry.2,8,10,25 Conversely, some studies suggest that more severe cases may demonstrate greater absolute correction but often require longer treatment durations.12,25 Given the mixed evidence, it remains unclear whether the improved discharge measurements observed in the intervention group were attributable to CMT or to lower baseline severity.
The mean age of helmet therapy initiation in this study was six months, which is within the commonly recommended therapeutic window of between 4 and 6-7 months.1,2,6-8 Although earlier initiation is generally associated with greater rates of correction,1,2,6,8,10 satisfactory outcomes have been reported when treatment begins before nine to ten months of age.10 Importantly, no significant difference in initiation age was observed between groups, supporting comparability and reducing the likelihood of age acting as a confounding factor.
The sex distribution in this study reflects reported epidemiological trends, with a slight predominance of male infants.1-3,8,9,12-16,18,22,27,29 Sex is generally considered a weak predictor of treatment outcome, and the balanced male-to-female ratio in this study supports generalizability across sexes.9,12
Helmet therapy is widely accepted as an effective intervention for moderate to severe positional plagiocephaly.1,2,6,8-10,12,24,25 Debate remains regarding its use in mild to moderate cases, with some guidelines recommending conservative management prior to orthotic intervention.5,6,9,12,17 The present study’s sample group fell within the moderate severity range, which is the most debated category as it lies on the boundary of arguments both for and against helmet therapy. Both groups demonstrated significant improvement, supporting the effectiveness of helmet therapy in this population. Interpretation is limited by the absence of data regarding conservative therapies received prior to helmet initiation.
Although CMT did not influence treatment duration, improvements in cranial symmetry outcomes were observed. Within the South African context, chiropractic care is frequently accessed by parents for pediatric conditions.21 A recent survey reported that approximately 36% of chiropractors in South Africa primarily focus on pediatric or family wellness practice.21 Furthermore, Doucet et al.22 identified torticollis and cranial asymmetries among the most commonly managed conditions by chiropractors treating children aged 0–23 months. Given that torticollis is a recognized risk factor for positional plagiocephaly,3-5,27 chiropractors may be well positioned to contribute to interdisciplinary management alongside orthotists, pediatricians, and physiotherapists.
Potential mechanisms underlying the observed findings include improvements in cervical mobility, reduction of muscular imbalance or torticollis, and facilitation of more symmetrical head positioning during periods of rapid cranial growth, as proposed in osteopathic and chiropractic literature.9,13,16,18,29,30 While these mechanisms remain theoretical within the context of this study, they may help explain the improved discharge symmetry observed in the intervention group.
Several limitations must be acknowledged. The small sample size limits statistical power and increases the risk of Type II errors. The retrospective design restricted control over potential confounders, including initiation age, baseline severity of asymmetry, infant growth rate variability, parental compliance with helmet wear, and the absence of standardized documentation regarding chiropractic treatment protocols. These variables were not formally adjusted for in the analysis, which may limit interpretability of the findings. Data were derived from a single orthotic practice, which may further limit generalizability. Strengths of this study include the use of precise three-dimensional cranial measurements, clinically relevant inclusion criteria, equal group sizes, and balanced sex distribution.
Chiropractic-specific research on positional plagiocephaly remains limited. Existing studies have relied on less precise measurement methods, such as diagonal calipers or tape measures, which may compromise measurement validity.29,30 This study contributes preliminary evidence using objective three-dimensional imaging and is among the first to examine CMT in conjunction with helmet therapy. Although no reduction in treatment duration was observed, the findings support further investigation into whether manual therapies may enhance cranial symmetry outcomes.
Future research should involve larger prospective studies or randomized controlled trials with standardized chiropractic protocols and multi-site recruitment. Such designs would improve statistical power, reduce confounding, and clarify the role of chiropractic manipulative therapy within interdisciplinary care models for positional plagiocephaly.
Conclusion
This study found that adding CMT during helmet therapy did not significantly reduce treatment duration but was associated with slight improvements in CVA and CVAI measurements of cranial asymmetry in this sample of patients presenting with positional plagiocephaly.
Acknowledgements
The author would like to thank the orthotist involved for granting access to clinical records and serving as gatekeeper to the retrospective data, as well as the orthotic assistants for their assistance with participant contact and survey dissemination.
References:
1. Çevik S, Isik S, Özkiliç A. The role of age on helmet therapy in deformational plagiocephaly and asymmetric brachycephaly. Childs Nerv Syst. 2020;36(4):803-810. doi:10.1007/s00381-019-04354-2.
2. Kim J, Kim J, Chae KY. Effectiveness of helmet therapy for infants with moderate to severe positional plagiocephaly. Clin Exp Pediatr. 2024;67(1):46-53. doi:10.3345/cep.2023.00626.
3. Cabrera-Martos I, Ortigosa-Gómez SJ, López-López L, Valenza MC, Valenza-Demet G, Ruiz-Extremera A. Physical therapist interventions for infants with nonsynostotic positional head deformities: a systematic review. Phys Ther. 2021;101(8):pzab106. doi:10.1093/ptj/pzab106.
4. Jung BK, Yun IS. Diagnosis and treatment of positional plagiocephaly. Arch Craniofac Surg. 2020;21(2):80-86. doi:10.7181/acfs.2020.00059.
5. The Royal Children’s Hospital Melbourne. Positional plagiocephaly [Internet]. Parkville (Australia): The Royal Children’s Hospital Melbourne; [cited 2025 May 26]. Available from: https://www.rch.org.au/clinicalguide/guideline_index/Positional_plagiocephaly/.
6. Corte AD, Rohde MA. Use of orthotic helmets in children with positional plagiocephaly and brachycephaly: a systematic review. Childs Nerv Syst. 2025;41(1):163. doi:10.1007/s00381-025-06826-0.
7. Marshall JM, Shahzad F. Safe sleep, plagiocephaly, and brachycephaly: assessment, risks, treatment, and when to refer. Pediatr Ann. 2020;49(10):e440-447. doi:10.3928/19382359-20200922-02.
8. Graham T, Adams-Huet B, Gilbert N, Witthoff K, Gregory T, Walsh M, et al. Effects of initial age and severity on cranial remolding orthotic treatment for infants with deformational plagiocephaly. J Clin Med. 2019;8(8):1097. doi:10.3390/jcm8081097.
9. Pastor-Pons I, Lucha-López MO, Barrau-Lalmolda M, de-la-Fuente Anuncibay R, Montes-Montes R, López-Rodríguez I, et al. Efficacy of pediatric integrative manual therapy in positional plagiocephaly: a randomized controlled trial. Ital J Pediatr. 2021;47(1):132. doi:10.1186/s13052-021-01079-4.
10. Kim MJ, Kang MK, Deslivia MF, Kim YO, Choi JW. Applicative factors of helmet molding therapy in late-diagnosed positional plagiocephaly. J Korean Med Sci. 2020;35(36):e295. doi:10.3346/jkms.2020.35.e295.
11. Fenton R, Gaetani SA. A pediatric epidemic: deformational plagiocephaly/brachycephaly and congenital muscular torticollis. Contemp Pediatr. 2019;36(2):1-8. https://www.contemporarypediatrics.com/view/pediatric-epidemic-deformational-plagiocephalybrachycephaly-and-congenital-muscular.
12. González-Santos J, González-Bernal JJ, De-la-Fuente Anuncibay R, Lucha-López MO, Barrau-Lalmolda M, López-Rodríguez I, et al. Infant cranial deformity: cranial helmet therapy or physiotherapy? Int J Environ Res Public Health. 2020;17(7):2612. doi:10.3390/ijerph17072612.
13. Panza R, Piarulli F, Rizzo V, Pasquarelli L, Merlino F, Montalto G, et al. Positional plagiocephaly: results of the osteopathic treatment of 424 infants. Ital J Pediatr. 2024;50(1):166. doi:10.1186/s13052-024-01729-3.
14. Kim DH, Kwon DR. Neurodevelopmental delay according to severity of deformational plagiocephaly in children. Medicine (Baltimore). 2020;99(28):e21194. doi:10.1097/MD.0000000000021194.
15. Blanco-Diaz M, Marcos-Alvarez M, Escobio-Prieto I, García-Alonso J, López-González L, Martínez-Villa L, et al. Effectiveness of conservative treatments in positional plagiocephaly in infants: a systematic review. Children (Basel). 2023;10(7):1184. doi:10.3390/children10071184.
16. Bagagiolo D, Priolo CG, Favre EM, Martinez R, Canterino C, Rossi D, et al. A randomized controlled trial of osteopathic manipulative therapy to reduce cranial asymmetries in young infants with nonsynostotic plagiocephaly. Am J Perinatol. 2022;39(S01):S52-62. doi:10.1055/s-0042-1758723.
17. Flannery AM, Tamber MS, Mazzola C, Klimo P Jr, Baird LC, Tyagi R, Bauer DF, Beier A, Durham S, Lin AY, McClung-Smith C, Mitchell L, Nikas D. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines for the Management of Patients With Positional Plagiocephaly: Executive Summary. Neurosurgery. 2016;79(5):623-624. doi: 10.1227/NEU.0000000000001426.
18. Cabrera-Martos I, Valenza MC, Valenza-Demet G, Benítez-Feliponi A, Robles-Vizcaíno C, Ruiz-Extremera A. Effects of manual therapy on treatment duration and motor development in infants with severe nonsynostotic plagiocephaly: a randomized controlled pilot study. Childs Nerv Syst. 2016;32(11):2211-2217. doi:10.1007/s00381-016-3200-5.
19. Hillyar CRT, Bishop N, Nibber A, Bell-Davies FJ, Ong J. Assessing the evidence for nonobstetric risk factors for deformational plagiocephaly: systematic review and meta-analysis. Interact J Med Res. 2024;13:e55695. doi:10.2196/55695.
20. Parnell Prevost C, Gleberzon B, Carleo B, Anderson K, Cark M, Pohlman KA. Manual therapy for the pediatric population: a systematic review. BMC Complement Altern Med. 2019;19(1):60. doi: 10.1186/s12906-019-2447-2.
21. Naidoo S, Hoenselaar NK, Yelverton C. Chiropractic attitude and utilisation of evidence-based practice in South Africa: a secondary analysis. Chiropr Man Therap. 2024;32(1):13. doi: 10.1186/s12998-024-00534-3.
22. Doucet C, Dubuc É, Imbeau C, Pohlman KA, Blanchette MA. Chiropractic pediatric patient management and interdisciplinary collaboration: a descriptive cross-sectional study of chiropractors in Quebec. Chiropr Man Therap. 2022;30(1):54. doi:10.1186/s12998-022-00464-y.
23. STROBE Statement. STROBE checklists [Internet]. Bern (Switzerland): University of Bern; 2007 [cited 2025 June 01]. Available from: https://www.strobe-statement.org/checklists/.
24. Lamberta LK, Murray TR, Gehred A, Weisleder P. Helmet therapy for positional plagiocephaly: a systematic review of the tools used to diagnose, offer treatment recommendations, and assess treatment outcomes of the condition. Pediatr Neurol. 2024;161:125-131. doi:10.1016/j.pediatrneurol.2024.09.007.
25. Hauc SC, Long AS, Rivera JC, Desai SC, Dhiman N, Fogel AL, et al. Predictive factors of outcomes in helmet therapy for deformational plagiocephaly and brachycephaly. J Craniofac Surg. 2023;34(1):231-234. doi:10.1097/SCS.0000000000009048.
26. Orthomerica. Product category/SmartSoc [Internet]. 2025 [cited 2025 Apr]. Available from: https://orthomerica.com/product-category/smartsoc/.
27. van Cruchten C, Feijen MMW, van der Hulst RRWJ. Demographics of positional plagiocephaly and brachycephaly; risk factors and treatment. J Craniofac Surg. 2021;32(8):2736-2741. doi:10.1097/SCS.0000000000007811.
28. Munabi NCO, Nelson MS, Francis SH. Risk factors for delayed diagnosis of positional plagiocephaly: a review of 25,322 patients. Cleft Palate Craniofac J. 2024;61(10):1679-1686. doi:10.1177/10556656231179068.
29. Douglas NA, Browning M, Miller J. Chiropractic care for the cervical spine as a treatment for plagiocephaly: a prospective cohort study. J Clin Chiropr Pediatr. 2017;15(3):1274-1279.
30. Gordon BD. A retrospective study of the management of deformational plagiocephaly with chiropractic care. Chiropr J Aust. 2017;45(2):155-174. Available from: https://research-ebsco-com.aecc.idm.oclc.org/linkprocessor/plink?id=a79dd98a-7fe4-3cc7-b917-55638fb510e8.
|
