| |
Clinical Close-up: Witteveen-Kolk Syndrome in a Three-Year-Old
Celeste Krawchuk, DC, DICCP (drclst@yahoo.com)
Amanda Hartman, CLC, BEC (amandak1017@gmail.com)
Witteveen-Kolk Syndrome (WITKOS) is a rare genetic disorder that shows mutations in the SIN3A gene. It has been labeled as a neurodevelopmental syndrome and as of 2020, around 40 individuals with WITKOS have been identified with a 1:1 male to female ratio.1 There are several ways that WITKOS may present, including intellectual disabilities (mild to moderate), developmental delays, short stature and dysmorphic facial features that may include a broad high forehead, long face, depressed nasal bridge, small mouth, malformed ears and a high palate.1,2 The SIN3A gene is a switch receptor for micro deletions. These patients may present with latching and feeding difficulties, behavioral issues, hyperlaxity in the joints and hypotonicity of their muscles.1
The mother of the patient was under chiropractic care with the author throughout her pregnancy. The fetus was active and in the vertex position through the third trimester. Mom was treated the day she went into labor and her midwife, doula and chiropractor palpated the fetus in the vertex position, but during labor he flipped into a breech presentation. He was a breech delivery accomplished at home, but had a difficult time latching, so the chiropractor was asked to adjust him at 13 hours old. When first assessed, he presented with overall low muscle tone. His suck swallow breathe (SSB) synchrony was disorganized. Oral evaluation revealed that he had a high palate, a tongue tie and upper lip tie. His upper cervical spine (C1 and C2) and his sacrum were subluxated and his cranial bones were not moving freely at the temporals, sphenoid and occiput. In addition, his mandible was retracted. Fingertip pressure was applied to adjust C1, C2 and the sacrum and craniosacral technique was applied to release the listed cranial restrictions. He immediately latched more deeply and securely to breast feed. He was adjusted again two days later at the same vertebral levels and the same cranial bones. When breast feeding, per his mother, he would latch well, then would tire quickly, with his jaw/mandible dropping due to muscle fatigue. Adjustments and CST would help with this temporarily. At three days old he had his ties lasered by a pediatric dentist. He was able to latch but continued to have poor milk transfer. Mom continued to attempt breastfeeding, but ended up pumping and bottle feeding, while working on his latch.
With continued chiropractic care, physical therapy, occupational therapy, speech therapy and feeding therapy he has been steadily improving. (see mother’s detailed account of obtaining a diagnosis of WITKOS). The patient is now three years old, walking, talking (but was delayed in speech development) and interacting appropriately for his age.
In June 2024, a set of twins were born to the same family and twin B presented with the same facial characteristics and feeding issues as his WITKOS brother and, upon evaluation, was given the same diagnosis. Twin A did not seem to carry the gene variation The author was able to adjust him within less than 10 hours of birth and found that he was also hypotonic, had a high palate and tired easily and quickly while breast feeding with a weak and insecure latch. After each adjustment and cranial session, his latch and feeding with a bottle would greatly improve for several days. The parents immediately enrolled him in speech, OT and PT, along with continued adjustments and his breastfeeding efficiency improved.
 |
 |
 |
 |
 |
| Cayman at 6 months, demonstrating his hyper-mobility and hyper-flexibility |
Cayman at 12 months, demonstrating his high palate. |
Cayman at 15 months, demonstrating his high forehead and dysmorphic facial features. |
Cayman at 36 months, demonstrating his elongated face. |
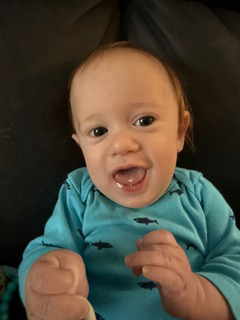
Photograph is of Oakley (*Twin B) at 4 months demonstrating his high forehead and elongated face. |
Mother’s Story:
We knew from birth that Cayman was hypermobile and hypotonic. After my water broke during labor, he flipped into a breech position but was born safely at home. In the hours and days after birth we saw how his cheeks, arms, and legs were all low tone. As a lactation consultant, I started suck training right away and supplementing with expressed milk in syringes. Our chiropractor came to our house 13 hours after birth and adjusted him for the first time and we both noted his tongue tie, upper lip tie, and extremely high and narrow palate that ascending into his nasal cavity. At three days old he had his ties lasered by a pediatric dentist. He was able to latch but continued to have poor milk transfer.
As the weeks went by, the most he would transfer at the breast was 1oz. After weeks of latching, pumping, and bottle feeding, I had a massive oversupply and chose to mostly pump for him and only latch on occasion. Latching was hard work for him and he needed cheek and chin support and he fatigued very easily. At eight weeks old, he had a three-day hospital stay for a UTI and while there, the pediatrician first heard his heart murmur. An echo led to a diagnosis of mild pulmonary artery stenosis and a tiny atrial septal defect. Both were very mild and would be monitored once a year. Cayman had an undescended testicle that was surgically repaired at one year old although both testes are still abnormally small. Cayman has always been small and below the first percentile for weight. His head and height are both below the 10th percentile. For the first year of his life, he met his developmental milestones on time.
Cayman did well with the introduction of purées but struggled with solid food. We started feeding therapy which lasted for six months. Around the same time, we also started speech therapy, occupational therapy, and physical therapy. Around two-and-one-half years old we started noticing absent seizures, predominantly at nighttime. Cayman didn’t develop his pincer grasp until almost three years old and at three years old he is developmentally a two-year-old. He has over 100 words (expressive language) and is starting to combine words. His hypotonia makes him extra clumsy and he falls multiple times a day.
We started exploring genetic testing first with Cayman’s older brother Malakai who is Autistic and has ADHD. Malakai has a deletion on the 15th chromosome and with Cayman’s history we had him tested next. Cayman’s genetic results came back with the same deletion on the 15th chromosome and a new variant of the SIN3A gene. When the genetics team first called with the results, they stated they had never seen it before in their own practice and there were only 30 documented cases in the world. Any variation of the SIN3A gene has been given the name Witteveen Kolk Syndrome. After being diagnosed, more tests were run and it was found that Cayman’s growth hormone was low which matched his lack of progress.
There are now over 50 known cases and a Facebook group for Witteveen Kolk families. With such a rare syndrome we learn more about it from each other and bring that information back to each team of doctors.
Fast forward and now we have five-month-old twins. Twin B, Oakley, looks like Cayman’s miniature clone. He’s hypotonic which we again noticed at birth although he wasn’t breech. He has the same facial features as Cayman. We immediately started physical therapy, occupational therapy, and speech therapy. His feeding journey has not been as complex as Cayman’s was. For the first couple of months, he leaked large puddles of milk whether at the breast or being bottle fed. He needed suck training and both cheek and chin support when feeding. He transferred milk better than Cayman did, especially when tandem feeding with his twin sister. From months one to five, we gradually moved from more pumping and bottle feeding to mostly latching at the breast. He no longer leaks milk and transfers well. He is also tiny and below the first percentile for weight. He failed his newborn hearing screen and we learned through his ABR test that he has severe hearing loss in his right ear that requires a hearing aid. While Witteveen Kolk Syndrome doesn’t present the exact same way in Cayman and Oakley, they both share many similarities with other Witteveen Kolk syndrome families.
Their father also has the same variant of the SIN3A gene and has a smaller stature and had developmental delays growing up. You can see similarities from the only study that exists for their syndrome here https://www.nature.com/articles/s41431-020-00769-7.
References:
1. “Knowledge on Rare Diseases and Orphan Drugs” Orphanet: Witteveen-Kolk Syndrom, Dec. 2020, https://www.eurogct.org/orphanet-portal-rare-diseases-and-orphan-drugs.
2. Van Dongen, Linde, Wingbermuhle, Ellen, Dingemans, alexander, Bos-Roubos, anja, Vermeulen, Karlijn, Pop-Purceleanu, Monica, Kleefstra, Tjitske, Egger, Jos (2020) Behavior and cognitive Functioning in Witteveen-Kolk Syndrome, American Journal of Medical Genetics, Vol. 182 Issue 10, Oct. 2020 pages 2384-2390. |
