Prognosis of patellofemoral pain in adolescents: a case report
By Heather A. Hanson, D.C., M.Sc
Abstract
Introduction: Patellofemoral pain is a common condition in adolescents and may significantly impact their activities of daily living. Methods: A literature search was performed using the PubMed database including the terms “knee pain,” “patellofemoral pain syndrome,” “patellofemoral pain,” and “anterior knee pain” combined with “prognosis” and “natural history.” Three relevant articles were identified including individuals aged 13-18 years. Case presentation: An active 14-year old female presented to the chiropractic clinic after being diagnosed with this condition by her general practitioner. The family wanted to know the long-term prognosis of the condition and if anything could be done, as the general practitioner had suggested that the condition would resolve on its own. Intervention: Home exercises were prescribed along with advice to temporarily suspend participation in physical education classes and consider orthotics. Soft tissue therapy and mobilizations of the knee joint were also applied. Outcomes: Despite these efforts, this patient continued to suffer from these complaints, though with reduced intensity, three years after the onset. Discussion: Three prospective studies examining the prognosis of this condition in a young population exist. Though heterogeneous in design, the evidence suggests that the course of patellofemoral pain in adolescents and young adults does not appear to be self-limiting in nature and its prognosis appears to be worse than that of other non-traumatic knee conditions. Conclusion: Early intervention appears to improve the chances of recovery, therefore chiropractors should be aware of this condition’s unfavorable prognosis and the urgency of initiating treatment in a timely manner.
Key Words: Patellofemoral pain syndrome, adolescent, knee pain.
Introduction
Knee pain is a common reason for which adolescents visit primary care providers,1 with patellofemoral pain affecting approximately 6-7% of adolescents, and accounting for almost half of adolescent knee complaints.2 The diagnosis of patellofemoral pain is made with peripatellar or retropatellar anterior knee pain of insidious onset provoked by activities such as long periods of sitting, kneeling, squatting, running and stair climbing.3
Traditionally, patellofemoral pain in adolescents has been regarded as a benign, self-limiting condition.4,5 However, one longitudinal study of female adolescents with patellofemoral pain showed that 78% continued to suffer from knee pain even after a long mean follow-up time of 16 years,6 indicating that the prognosis might not be as good as previously believed.
This work presents the case of an adolescent female presenting with patellofemoral pain, with consideration for the most recent evidence surrounding the prognosis of
this condition in adolescents.
Methods
A search of the literature was performed using the PubMed database. The following search terms were used: “knee pain,” “patellofemoral pain syndrome,” “patellofemoral pain” and “anterior knee pain” combined with the terms “prognosis” and “natural history.” Filters were used to limit the search to human studies of adolescents (ages 13-18 years). Hand searching of reference lists of relevant articles was also performed to identify additional relevant literature. Inclusion criteria included English language, publication between the years 2000 and 2019 and a prospective study design. Studies of a solely adolescent population were scarce, so it was decided that those including a young adult population (older than 18 years of age) along with adolescents (13-18 years of age) would not be excluded. In total, three relevant articles were identified.
Case Presentation
A 14-year old female presented with a new complaint of severe pain localized to the retropatellar area of her right knee at a consultation previously planned for maintenance care and monitoring of a scoliosis. There was no history of trauma, but the patient was highly active, cycling approximately 40 kilometers every school day and swimming recreationally once per week.
Approximately four weeks after the onset, mother had consulted their general practitioner, who told them her pain was related to growth and would simply resolve on its own, not offering any further treatment options. At their next planned chiropractic appointment approximately two weeks after consulting the general practitioner, the family wanted to know whether chiropractic treatment could be of benefit for these complaints and whether the general practitioner’s opinion about the complaints was correct.
Evaluation
No swelling or redness was visible, and pain was reproduced with patellar compression and palpation of the medial articular surface of the patella. An obvious pes planus deformity was present, with slight adduction and internal rotation of the thighs when standing.
Intervention and Outcomes
As a first step in approaching her complaint, the patient was provided with home exercises for her quadriceps, with particular focus on strengthening of the vastus medialis muscle. Since her transport to school required cycling, advice was given to stop participation in physical education classes for at least the next two weeks in order to allow some of the irritation to subside. A subsequent visit was scheduled at the usual interval of care, two months later, with the expectation that the knee pain would have diminished by then. At that moment, no obvious reason seemed present to lead one to expect that her complaint might become chronic.
At the next visit, the complaints had not resolved. Since the pain remained quite intense and an obvious pes planus deformity was present, a suggestion was made to consider having orthotics made by another practitioner. Soft tissue therapy for the vastus medialis and popliteus muscles and mobilizations of the knee joint were also applied. Due to other circumstances, her next appointment took place five months later. While it was hoped that physical rest during the summer vacation might have helped in her recovery, not much progress had been made. She admitted to very rarely doing her home exercises, but said that this was because the exercises were too painful to complete. As a result, more emphasis was put on proximal exercises for the hip musculature, which have been found to be effective in more recent studies7 and were less painful for her to complete. (See Table 1.)
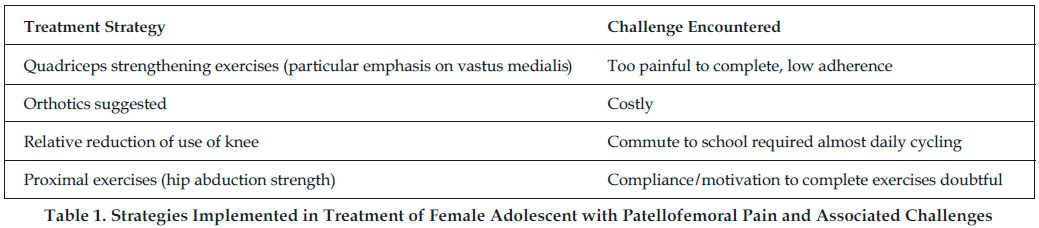
Her mother was also encouraged to try to monitor the home exercises. These changes resulted in greater compliance with the home exercise program and ultimately a decrease in the patient’s subjective pain level. While able to continue participating in swimming, she also admitted that she limited the intensity with which she took part as a result of the pain. At follow-up three years after her initial presentation with this complaint, the patient reported some remaining symptoms, though these were mild in frequency and severity.
Discussion
The identified evidence is clear that while some patients with patellofemoral pain recover, a large proportion of affected adolescents and young adults continue to experience pain and disability in the long term and that the prognosis for patellofemoral pain tends to be worse than for other non-traumatic knee conditions.8,9,10 (See Table 2).
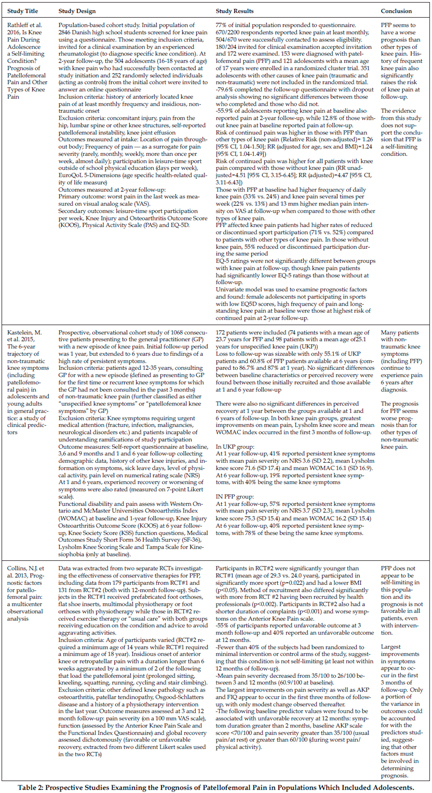
When followed over a two-year period, adolescents with patellofemoral pain had a significantly higher risk of continued pain than subjects with other types of knee pain (Relative risk (RR) of knee pain at follow-up=1.26 (95% CI, 1.05-1.50).10 They also reported more frequent and intense pain at follow-up than the subjects with other types of knee pain, though all types of baseline knee pain raised the risk of knee pain at follow-up (RR=4.51 (95% CI, 3.15-6.45)).10 Similarly, a longitudinal study of adolescent and young adult patients showed a worse prognosis for patellofemoral pain patients, with 40% experiencing persistent symptoms and only 19% of patients with unspecified knee symptoms experiencing persistent pain six years after study.9 Therefore, the evidence does not appear to support the assertion that patellofemoral pain is self-limiting. Rather, it suggests a high risk of chronicity for this condition.
Evidence also exists to suggest that the largest improvements in pain and functional outcomes for patellofemoral pain tend to occur during the first three months of follow- up8,9 which suggests that if patients are likely to recover either spontaneously or with treatment, that it will generally occur at an early stage. These findings point to the existence of a critical period in which interventions might have a better chance of success. Unfortunately, patients with non-traumatic onset of pain are known to be less likely to seek care.10 This, along with the erroneous belief that the condition is benign and self-limiting, are possibly barriers to the delivery of appropriate care and recovery.
When considering the relevant literature and the patient in this case, it did not appear that the information and advice that this family had received from their general practitioner was consistent with the current best evidence. Rather, the evidence seemed to suggest that early intervention was appropriate, rather than a “watch and wait” management style which would be indicated if this condition were truly self-limiting. A longer history of knee pain at baseline (more than two months of pain) has been identified as the most consistent predictor of poor outcome8,12 supporting the notion that early intervention may be desirable in order to attempt to avoid chronicity. Considering this knowledge, it seems that more frequent chiropractic appointments were probably indicated in the period following this patient’s presentation with this new complaint.
Exercise therapy is generally recognized as the mainstay of conservative treatment for patellofemoral pain, though the evidence for its efficacy is not of particularly high quality and focuses mainly on adults.13,14 Quadriceps exercises with a particular emphasis on the vastus medialis muscle, have traditionally been the most commonly used exercise approaches.15 Such exercises had been initiated with this patient. However, considering that her complaints had been present for a relatively long period before they were mentioned at a chiropractic appointment, this delay in initiating treatment might have negatively impacted her clinical outcome.
The response to exercise therapy in adolescents also seems to differ from that in older patients. One randomized trial using a physical therapy intervention demonstrated that 81% of patients aged 18-40 years reported moderate to marked improvement at 12 month follow-up on a global rating scale16 while similar interventions in a trial including patients aged 15-19 years resulted in only 38% self-reported recovery at 12 months.17 Adolescents have also been found to comply poorly with treatment recommendations. Low participation rates in supervised training sessions and low compliance rates with recommendations for home exercises were observed in the Rathleff (2015) trial, even though the study setting had significant supports in place to encourage compliance.17 However, those adolescents with the best home exercise adherence were found to have markedly better rates of clinical improvement (Odds ratio = 4.04, 95% C.I. 1.42 to 11.55).17 Clinicians may therefore need to find innovative ways to improve adolescent adherence to treatment, which could involve strategies such as involving parents in monitoring home exercises, restricting screen time until exercises are completed, scheduling more frequent in-office visits or using time in physical education classes to do exercises.
Further concern about this patient’s situation arose from the existence of some evidence suggesting that patellofemoral pain may have more serious long-term consequences. One theory suggests that anterior knee pain in early life may lead to osteoarthritis of the knee in adulthood18 with a retrospective study showing a strong relationship between anterior knee pain in young adulthood and development of patellofemoral osteoarthritis later in adulthood.4 A systematic review failed to identify sufficient high-quality evidence for a causal relationship, but concluded that the two conditions might at least have some shared biomechanical risk factors including alignment issues in the lower limb, patellar tracking issues and muscular dysfunction19 making it conceivable that this theory might be applicable at least in certain individual cases.
Some research suggests that there is cause for concern about the long-term effects of this pain condition on adolescent females in particular. Altered pain processing mechanisms resulting in higher sensitivity to pain have been found in patients with patellofemoral pain, suggesting that altered central or peripheral pain processing mechanisms may play a role in this condition, particularly in female.20,21 This is of concern, due to the potential of this mechanism to contribute to other generalized pain conditions.
Other important effects of knee pain have been recognized including lower health-related quality of life scores in the adolescent and pre-adolescent population21 and decreased activity levels in participation in sport.10,23 Adolescents suffering from patellofemoral pain are more likely to reduce their participation in sports than patients with other forms of knee pain.10 The risk of low physical activity levels may be of particular concern in the female adolescent population. Females are affected by knee pain at higher rates than males3,11 and girls tend to be less active than boys throughout childhood and adolescence, with rates of activity declining faster in girls than boys during the teenage years.24 This may have significant short and long term effects, as inactive teens may not achieve the activity levels required for them to reap the many recognized positive benefits on their physical and mental health.25 Furthermore, levels of physical activity in early life tend to track into adulthood, possibly leading to adult sedentariness which may raise the risk of chronic conditions like obesity, osteoporosis, cardiovascular disease and diabetes.26
Contrary to what the evidence suggested, there was little risk of low physical activity levels in this case, as eliminating her bicycle commute to school was not an option for this family.
The most widely accepted theory proposes that patellofemoral pain is caused by patellofemoral maltracking, causing increased stress on the patellofemoral joint, with various causes of patellar tracking issues proposed, generally involving muscular weakness or alignment issues in the lower limb.7,15 It seemed that a decrease in activity might actually be indicated in this patient’s situation, in order to limit irritation at the patellofemoral joint. As a result, advice was given to temporarily stop participating in physical education classes and where possible, abstain from other activities which aggravated her pain, while continuing her home exercises.
Conclusion
Treatment of patellofemoral pain in adolescents presents unique challenges and even with good quality treatment, it seems that the risk of chronicity remains great. Ideally, treatment aims to strike a balance between encouraging healthy movement and optimizing participation in sport and other physical activity while avoiding excessive irritation of the knee. Clinicians should be aware of the potential long-term effects of these types of complaints and attempt to tailor their treatment to the patient’s individual situation to achieve the best possible outcome.
References
1.Van der Linden MW, Westert GP, de Bakker DH, Schellevis FG. Tweede Nationale Studie naar ziekten en verrichtingen in de huisartspraktijk. Klachten en aandoeningen in de bevolking en in de huisartspraktijk. [online]. 2004. Utrecht: NIVEL.
2.Molgaard C, Rathleff MS, Simonsen O. Patellofemoral pain syndrome and its association with hip, ankle, and foot function in 16- to 18-year-old high school students: a single-blind case-control study. Journal of the American Podiatric Medical Association 2011; 101: 215-222.
3.Lankhorst NE, Bierma-Zeinstra SMA, van Middelkoop M. Risk Factors for Patellofemoral Pain Syndrome: A Systematic Review. Journal of Orthopaedic and Sports Physical Therapy 2012; 42(2): 81-94.
4.Utting MR, Davies G, Newman JH. Is anterior knee pain a predisposing factor to patellofemoral osteoarthritis? The Knee 2005;12(5): 362-365.
5.Rathleff MS. Patellofemoral pain during adolescence: much more prevalent than appreciated. British Journal of Sports Medicine 2016; 50: 831-832.
6.Nimon G, Murray D, Sandow M, Goodfellow J. Natural history of anterior knee pain: a 14- to 20-year follow-up of nonoperative management. Journal of Pediatric Orthopaedics 1998;18(1): 118-122.
7.Lack S, Barton C, Sohan O, Crossley K, Morrissey D. Proximal muscle rehabilitation is effective for patellofemoral pain: a systematic review with meta-analysis. British Journal of Sports Medicine 2015; 49: 1365-1376.
8.Collins NJ, Bierma-Zeinstra SMA, Crossley KM, van Linschoten RL, Vicenzino B, van Middelkoop M. Prognostic factors for patellofemoral pain: a multicenter observational analysis. British Journal of Sports Medicine 2013; 47: 227-233.
9.Kastelein M, Luijsterburg PAJ, Heintjes EM, van Middelkoop M, Verhaar JAN, Koes BW, Bierma-Zeinstra SMA. The 6-year trajectory of non-traumatic knee symptoms (including patellofemoral pain) in adolescents and young adults in general practice: a study of clinical predictors. British Journal of Sports Medicine 2015; 49: 400-405.
10.Rathleff MS, Rathleff CR, Olesen JL, Rasmussen S, Roos EM. Is Knee Pain During Adolescence a Self-limiting Condition? Prognosis of Patellofemoral Pain and Other Types of Knee Pain. American Journal of Sports Medicine 2016; 44(5): 1165-1171.
11.Rathleff MS, Skuldbøl SK, Rasch MN, Roos EM, Rasmussen S, Olesen JL. Care-seeking behavior of adolescents with knee pain: a population-based study among 504 adolescents. BMC Musculoskeletal Disorders 2013; 30(14): 225.
12.Collins NJ, Crossley KM, Darnell R, Vicenzino B. Predictors of short and long term outcome in patellofemoral pain syndrome: a prospective longitudinal study. BMC Musculoskeletal Disorders [online] 2010; 11:11. Available from: http://web.a.ebscohost.com/ehost/pdfviewer/pdfviewer?vid=2&sid=21782ffa-210f-4b6e-a522-6897cb15d5a2%40sessionmgr4010&hid=4206 [Accessed 10 October 2016].
13.Witvrouw E, Callaghan MJ, Stefanik JJ, Noehren B, Bazett-Jones DM, Willson JD, Earl-Boehm, JE, Davis IS, Powers CM, McConnell J, Crossley KM. Patellofemoral pain: consensus statement from the 3rd International Patellofemoral Pain Research Retreat held in Vancouver, September 2013. British Journal of Sport Medicine 2014; 48(4): 411-414.
14.Van der Heijden RA, Lankhorst NE, van Linschoten R, Bierman-Zeinstra SMA, van Middelkoop M. Exercise for treating patellofemoral pain syndrome: an abridged version of Cochrane Systematic Review. European Journal of Physical and Rehabilitation Medicine 2016; 52(1): 110-133.
15.Bolga LA, Boling MC. An update for the conservative management of patellofemoral pain syndrome: a systematic review of the literature from 2000 to 2010. International Journal of Sport Physical Therapy 2011; 6(2): 112-115.
16.Collins N, Crossley K, Beller E, Darnell R, McPoil T, Vicenzino B. Foot orthoses and physiotherapy in the treatment of patellofemoral pain syndrome: randomised clinical trial. BMJ [online] 2008; 337:a1735. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2572211/ [Accessed 20 October 2016].
17.Rathleff MS, Roos EM, Olesen JL, Rasmussen S. Exercise during school hours when added to patient education improves outcome for 2 years in adolescent patellofemoral pain: a cluster randomised trial. British Journal of Sports Medicine 2015; 49: 406-412.
18.Antony B, Jones G, Jin X, Ding C. Do early life factors affect the development of knee osteoarthritis in later life: a narrative review. Arthritis Research and Therapy [online] 2016; 18: 202. Available from: http://arthritis-research.biomedcentral.com/articles/10.1186/s13075-016-1104-0 [Accessed 1 October 2016] .
19.Thomas MJ, Wood L, Selfe J, Peat G. Anterior knee pain in younger adults as a precursor to subsequent patellofemoral osteoarthritis: a systematic review. BMC Musculoskeletal Disorders [online] 2010; 11: 201. Available from: http://web.a.ebscohost.com/ehost/pdfviewer/pdfviewer?vid=6&sid=21782ffa-210f-4b6e-a522-6897cb15d5a2%40sessionmgr4010&hid=4206 [Accessed 1 October 2016].
20.Van der Heijden RA, Rijdertse MM, Bierma-Zeinstra MA, van Middelkoop M. Lower Pressure Pain Thresholds in Patellofemoral Pain Patients, Especially in Female Patients: A Cross-Sectional Case-Control Study. Pain Medicine 2018; 19: 184-192.
21.Holden S, Straszek CL, Rathleff MS, Petersen KK, Roos EM, Graven-Nielsen T. Young females with long-standing patellofemoral pain display impaired conditioned pain modulation, increased temporal summation of pain, and widespread hyperalgesia. Pain 2018; 159(12):2530-2537.
22.Rathleff CR, Olesen JL, Roos EM, Rasmussen S, Rathleff MS. Half of 12-15-year-olds with knee pain still have pain after one year. Danish Medical Journal [online] 2013; 60(11):A4725. Available from: http://www.danmedj.dk/portal/page/portal/danmedj.dk/dmj_forside/PAST_ISSUE/2013/DMJ_2013_11/A4725 [Accessed 3 October 2016].
23.Witvrouw E, Lysens R, Bellemans J, Cambier D, Vanderstraeten G. Intrinsic Risk Factors For the Development of Anterior Knee Pain in an Athletic Population A Two Year Prospective Study. American Journal of Sports Medicine 2000; 28(4):480-489.
24.Dumith S, Gigante DP, Domingues MR, Kohl HW III. Physical activity change during adolescence: a systematic review and a pooled analysis. International Journal of Epidemiology 2011; 40(3):685-698.
25.Janssen I, LeBlanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity [online] 2010;7:40. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2885312/pdf/1479-5868-7-40.pdf [Accessed 15 October 2016].
26.Hallal PC, Victora, CG, Azevedo, MR, Wells, JC, Adolescent physical activity and health: a systematic review. Sports Medicine 2006; 36(12):1019-1030.
|
